Proper Imaging Reveals the Physical Damage from Concussion and TBI
BRINGING YOU CURRENT INFORMATION ABOUT HOW TO HELP TREAT AND HEAL BRAIN WOUNDS: CONCUSSIONS, TBI, PTSD
Advanced imaging is outpacing medicine’s ability to keep up with implications of the “new” brain science, and the nature of brain wounding. Medical textbooks are out-of-date with respect both to the nature of brain wounds and treatments to heal those wounds.
Drs. Carol Henricks and Paul Harch have put forward current scientific understandings.
Concussion: Not Just a Brain Bruise
Jun 30, 2022 08:00AM ● By Carol L. Henricks
Awareness of concussion injury exploded with the movie Concussion in 2015. The correlation between multiple concussions and neurodegenerative conditions was brought to the big screen. The common analogy of concussion being a “brain bruise” suggests that it is a minor injury that should recover in a few days without any permanent consequences. However, this is not true.
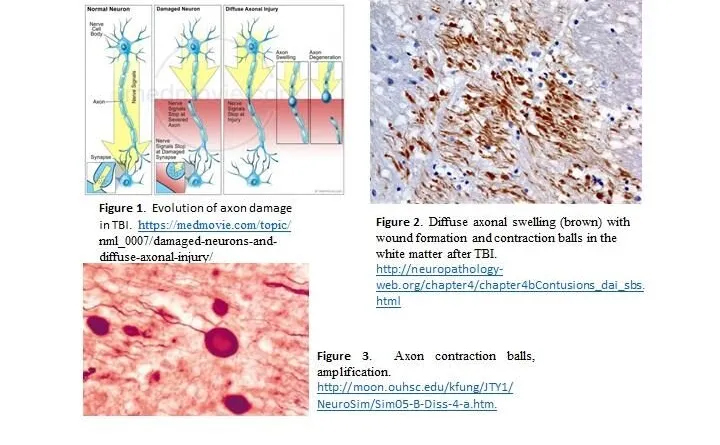
Our brains are uniquely designed and complex, more sophisticated than any computer. Every activity is a function of networks in the brain. The brain tissue injury that occurs as the result of concussion is complex and disruptive. Concussion is the result of many kinds of trauma that cause the brain to be shaken around inside the skull, causing diffuse axonal injury (DAI).
DAI creates lesions all throughout the brain, damaging the myelin (the fatty coating around axons), and may cause damage to deeper axonal structures. Diffuse injury disturbs network communication in the brain. Synapses—where one brain cell or neuron uses neurotransmitters to communicate with another brain cell—can be pulled apart, therefore disrupting cell-to-cell communication. The microenvironment of electrolytes and other brain-specific chemicals around the brain cells, glia and other support cells is disrupted and may effect electrical conductivity and functioning of cells.
Even a minor concussion may cause breaches in the blood brain barrier (BBB). A breach in the BBB allows chemicals, toxins and infections access to the brain when they would otherwise be blocked. The microtubular structure that internally organizes the neuron and allows transport of neurotransmitters to the synapse may be disrupted and disable cellular function.
Brain cells that are damaged and not restored to function begin a process of degeneration; this dying back of the cell leads to cell death and brain atrophy. This is the definition of a neurodegenerative process. Neurodegenerative processes include dementia, Parkinson’s disease and ALS.
Functional recovery—restoring the ability to read, sleep and balance, visual function and depth perception, cognitive activities and more—can be addressed by therapy, where some re-wiring and re-networking of the brain may occur. However, decline may still occur because functional recovery is different from biologically and physiologically healing the brain.
Military veterans, first responders and athletes in contact sports are at great risk for concussion and recurrent concussion, which causes cumulative injury and a high risk for neurodegenerative conditions. Traditional Brain MRI sequences, even with contrast, do not aid in diagnosing concussion because they do not highlight the disconnections. Brain MRI – DTI (diffusion tensor imaging) sequencing and/or Brain Quality SPECT scanning are the imaging tools of choice. Objective computer-based functional testing, including the RightEyeQ test (a standardized objective test of visual fixation and follow), reaction time testing and formalized balance testing, are objective and predictive, which is a good way to establish a baseline. Take brain health seriously and pursue meaningful testing and active treatment for concussion.
Carol L. Henricks, M.D. is a neurologist specializing in the use of hyperbaric oxygen therapy (HBOT) and PEMF at NorthStar Hyperbaric, in Tucson. (HBOT) saturates the body with oxygen, reducing inflammation and enhancing recovery from central nervous system injury. Connect at 520-229-1238 or NorthStarHBOT.com.
Dr. Paul Harch has cleared up the confusion In a seminal Meta Analysis: Systematic Review and Dosage Analysis: Hyperbaric Oxygen Therapy Efficacy in Mild Traumatic Brain Injury Persistent Postconcussion Syndrome.
TBI (5, 6) is a heterogeneous (7–27) diffuse physical injury to the brain that causes mechanical (7, 8, 28, 29) disruption of gray (22–24, 30, 31) and white (10, 15, 22, 23, 30, 32–35) matter, ischemia (36), hypoxia (29, 37, 38), edema (29, 39, 40), vasospasm (41, 42), release of neurochemicals (43, 44), and reperfusion injury (39, 45) and affects over 4.1 million people annually in the U.S. alone (46). These gray and white matter wounds in both blunt (10, 11) and blast TBI (22, 24) mature with time, resulting in the downstream synaptic loss (9, 23, 47), nerve cell loss (10, 11), and overall tissue loss (25–27, 48). This chronic tissue pathology is responsible for permanent postconcussive symptoms in over 15% of mTBI patients (49–51) and has been paradoxically designated a psychiatric condition, PPCS (2). Treatment has consisted of adaptive, stimulative, or accommodative approaches with limited evidence of efficacy (52–54). None of them address the biological repair of the underlying gray and white matter wounds.
Hyperbaric oxygen therapy (HBOT) has been historically defined as treatment with 100% oxygen at a minimum arbitrary pressure of 1.4 atmospheres absolute (ATA) (55, 56) for a narrow list of acute and chronic wound conditions (56). The U.S. Food and Drug Administration (FDA) has categorized HBOT as a prescription medical gas (oxygen) consisting of increased barometric pressure and hyperoxia (57). It has been scientifically defined as “a medical treatment that uses increased atmospheric pressure and increased oxygen as drugs by fully enclosing a person or animal in a pressure vessel and then adjusting the dose of the drugs to treat pathophysiologic processes of the diseases” (58). Based on this scientific definition HBOT can be appreciated as a treatment for common acute and chronic wound pathophysiology (56, 58–60) found in acute and chronic wound conditions (56, 58–62).
Hyperbaric oxygen therapy (HBOT) has been applied to chronic TBI wounds in animals and humans since 1989 (46, 63–98) with apparently conflicting results for mTBI (46, 66–89, 99–105). Various researchers have attributed the different results to mischaracterized sham groups/the effects of different doses of HBOT (46, 80, 99–105), design differences (106), (small sample size, dissimilar outcome measures/populations/sites/protocol adherence, non-equivalence of groups, selection bias) (73, 81), ritual experience (75), and placebo/Hawthorne effects (107). The conflict stems from control group selection based on the historical definition of HBOT (55) where the bioactivity of barometric pressure and <100% oxygen were dismissed.
This systematic review of the science and literature on HBOT in mTBI PPCS analyzes the studies/data based on the scientific definition of HBOT (58) and the U.S. FDA’s classification of HBOT as a dual-component drug (57). Recognizing that the HBOT studies consist of different doses of increased pressure and hyperoxia, the evidence is ranked according to the Evidence-Based Medicine hierarchy of evidence for treatment in clinical studies (3). The analysis demonstrates Level I evidence for the efficacy of 40 HBOTs at 1.5 ATA of oxygen (46, 75) in the treatment of blast or blunt mTBI/PPCS.